Ebola Response: ASLM Interview with Dr. Jean-Bosco Ndihokubwayo
Ebola Response:
ASLM Interview with Dr. Jean-Bosco Ndihokubwayo, WHO-AFRO Regional Focal Point
On behalf of ASLM, Dr. Paula Fernandes interviews Dr. Jean-Bosco Ndihokubwayo, World Health Organization (WHO) Regional Focal Point, WHO Regional Office for Africa (WHO-AFRO), about his involvement in the WHO response to the Ebola outbreak in West Africa.
Original interview date: 10 June 2014
Disclaimer: Any views or opinions presented in this interview are solely those of the interviewee and do not necessarily represent those of any organisation.

Dr. Bosco, you were heavily involved in the recent Ebola outbreak. Can you tell us about your roles and responsibilities within the WHO?
Dr. Jean-Bosco Ndihokubwayo (JBN): I was appointed as General Technical Coordinator of WHO efforts to help the government of Guinea to control the on-going Ebola outbreak that started early in December 2013. So my frame of reference was to ensure that all the WHO teams that were sent to the ground are working in a coordinated and sustainable manner so that we can have good results.
How did you first hear about the Ebola outbreak?
JBN: The Ebola outbreak in Guinea, we heard about it in February 2014, but as usual this kind of disease starts earlier than when we know about it. This is because of surveillance issues that we’re facing in the region and in nearby countries. The outbreak started in December 2013, and it was confirmed on 21 March 2014 by the Guinean government. Blood samples had to be collected [to confirm the outbreak]; 20 samples were collected from patients and 15 of the 20 samples came back positive for Ebola.
Is this a normal amount of time you’d expect before you got laboratory confirmation?
JBN: The laboratory worked very, very fast, because the specimens were sent on the 19th of March; the confirmation came back the 21st of March. So it was just 48 hours. They did extremely well, and this is in accordance with the International Health Regulation requirements concerning the lab confirmation of a public health event such as the Ebola Virus Disease Outbreak in Guinea.
Is this the normal amount of time one would expect from first case to notification by the country?
JBN: The first case was notified exactly on the 26th of December. The incubation period is 21 days. When Ebola starts to affect an area, given the symptoms, it looks like malaria or any other disease with fever as major symptom. But the government of Guinea had some concerns when three health care workers passed away with the same symptoms as the patients they were treating. And this is how they came to know that this is something different—it’s not malaria, it’s not a mysterious disease—it may be a haemorrhagic fever disease. And it was Ebola virus, unfortunately.
So, when you first received the news, how did you get the information? Did someone call or email?
JBN: It is the responsibility of the country to declare an outbreak, and this is what Guinea did on the 21st of March. And the WHO was immediately called to [provide] support. I was not the first to go there, but I was part of the second team, trying to coordinate all the ongoing efforts to control the Ebola outbreak in Guinea.
How many partners are there and how are efforts coordinated?
JBN: Many partners. For example, we had the CDC, the Red Cross; we had other partners like Médicins Sans Frontières (MSF), of course, for case management and patient management, and other partners as well. There were at least 10-15 partners, and all the partners were working under WHO leadership. I was there to ensure that WHO leadership is assured in terms of coordination of efforts to overcome the Ebola Virus Disease outbreak.
Can you describe the steps taken in response to an outbreak?
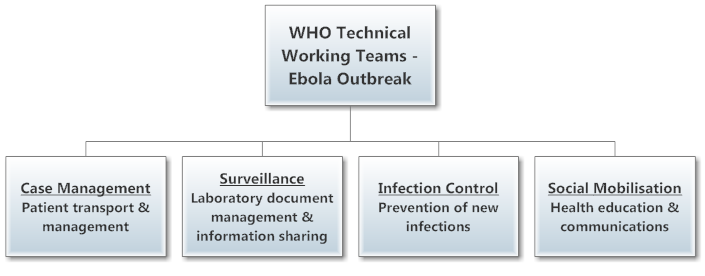
JBN: It is the responsibility of the coordinator to establish and monitor the teams, what we call technical working teams: on surveillance, which includes laboratory document management, collection and transportation of samples to the laboratories, laboratory processing of the samples and release of laboratory results; on case management, which includes the transportation of patients; and on infection control, which is more than important when it comes to Ebola, and when it comes to managing the patients that pass away, which have to be safely buried by professional teams that are well trained to do so.
It is the responsibility [of the infection control team] to train the healthcare workers on how to protect themselves against Ebola. Unfortunately, in this outbreak, the healthcare workers paid a heavy cost in the affected countries in West Africa, including Guinea, Liberia, Nigeria and Sierra Leone. Ebola has been a real disaster for the healthcare workers, and this is the first time in the history of Ebola that we’ve lost so many nurses, doctors, et cetera. The infection control team also keeps the families from touching the bodies, because the bodies are very dangerous and it is during the burial ceremonies that many people can get infected if they are not well-informed and protected.
We also had another team working on social mobilisation. Social mobilisation is a very important part of Ebola outbreak management because the populations in the affected regions have to understand the crucial roles they have in protecting themselves and their families, and also in fully cooperating with the Ebola prevention teams in the ground by informing them about suspected patients and their contacts as well as about people who have died in the community from an unknown disease. The populations living in the affected districts are key in organising what we call community-based surveillance; if the populations don’t collaborate and provide information, it is unfortunately extremely difficult, nearly impossible, to control the Ebola outbreak.
I wanted to ask a question about social mobilisation. In a situation where you have an Ebola outbreak, presumably the people who are close to the infected patient are very afraid of the disease. Do they try to hide suspicious deaths? What are the cultural implications of such an outbreak?
JBN: That is a problem, especially with Guinea. Some communities are trying to deny that this is another outbreak, saying that this is not an Ebola outbreak. The reason why is that they want to touch the patients, they want to care for patients, but this is very dangerous. And really, this is where we are having problems, and this is where we are trying to help with information mobilisation, to let the people know that touching an Ebola patient and his family will cause problems. It is very important to inform the population about the symptoms of Ebola, and also about the measures to protect themselves. This is what we’re doing right now, on the ground. Again, social mobilisation is a very important part of Ebola outbreak management because, as I said previously, the population has to have the right information and take the appropriate measures to protect themselves and to collaborate with healthcare workers and other stakeholders to put in place Ebola control measures.
Tell me a little bit about the dangers of collecting and transporting specimens.
JBN: This is a very important part of [disease] control, but fortunately we trained Guineans who work in labs on the ground on how to wear what we call personal protective equipment, and how to collect samples from patients and perform post-mortem sample collection. Because, for example, if someone passes away, and you don’t have information that he had Ebola, you may lose some aspect of Ebola surveillance. When someone is Ebola positive, you have to notify all the contacts he’s had, and follow-up with the contacts for 21 days because that is the incubation period of the disease. So, we trained the Guineans on how to collect the samples, save the samples, and ship the samples out to the mobile laboratories in Guinea.
Now, these mobile laboratories, are they set up as BSL-4 facilities?
JBN: They are BSL-3 facilities, using real-time PCR, plus serology to confirm. If real-time PCR is negative, potentially the sample was taken while the patient was non-viraemic, without Ebola virus appearing in the blood, and so we have to use serology testing to see if the patient has Ebola antibodies or not. What I observed when working on the ground is that the serology testing provides little added value when compared to real-time PCR; for example, out of 150 samples, only a few were RT-PCR negative and serology positive. When the RT-PCR is negative, it is likely that the Ebola serology testing will also be negative.
The laboratory is playing a critical role in the management of Ebola. It is the PCR result that determines whether a patient can be released from isolation to join his or her family. In fact, if the Ebola PCR becomes negative, this means that the patient is out of danger, that he is no longer viraemic or a danger to others and can be released from the hospital.
So, it is critical to obtain early diagnosis and isolate the patient to protect contacts and health workers?
JBN: Oh, yes, isolation is critical. To approach a patient with Ebola, you have to wear personal protective equipment. You know, everything has to be covered, including your eyes, your nose, everything. And the problem with this personal protective equipment is that it gets so hot inside that one can only really spend a maximum of one hour with the patient.
So have you worn this protective equipment?
JBN: Yes, I wore protective equipment when helping collect samples from patients, saliva samples from deceased patients, but also when following up the patients contacts that are not feeling well to ensure it is not the symptoms of Ebola Virus Disease that are starting.
What’s the interaction with patients like under the circumstances of patient isolation, given that the patient is terrified, and without their family?
JBN: You have to assure him, to let him know that you are a human being like him, and to let him know you will try your best to make sure he’s safe. You know, the most important thing to do for patients when they arrive, is to get them to drink water. They can drink up to seven litres of water in 24 hours. If they are not too badly sick, this will help them a lot.
As for the families, we have windows in the isolation wards to let the patients see their relatives. We sometimes also help some family members of the patients wear PPEs (personal protective equipment) and go see their relatives who are sick and isolated. This is very important, so that [the family] knows we are caring for the patient. The local population is much more likely to collaborate with health workers when they understand what is going on. It is important to underline that when the patient arrives in the healthcare centre early in the disease, we have a greater chance of saving him from death. Up to 60% of the Ebola patients who come to the hospital can be saved. When I was in Conakry [Guinea], we had patients in the isolation ward who were relatively safe, as the mortality rate there was about 40%, which is really good compared to what happened, for example in Geckedou, another place that experienced an Ebola outbreak. In Gekidou, [the mortality rate] was up to 70%, as patients were coming very late, and on top of that they had other diseases, like malaria, because this area is endemic for malaria, and co-infections contribute to mortality risk.
So malaria/Ebola co-infection has a negative impact for recovery?
JBN: It’s very bad. And malnutrition is another factor which may be very bad for Ebola patients.
How does the close proximity of international borders impact the outbreak? What happens on the borders of these countries?
JBN: For example, the border between Sierra Leone and Guinea does not exist. That’s why we have an outbreak in Sierra Leone and in Guinea, because these are the same people, and they are relatives. You cannot stop relatives from visiting each other on the other side of the border. This is also what is happening in Liberia. This is a big problem, but what we can do is improve surveillance intervention activities at the borders. And this is what we are doing. We have teams in Sierra Leone, teams in Liberia, which are working closely with teams in Guinea, sharing information and sharing samples.
So, when you do transport specimens, what kinds of containers do you use?
JBN: We have strict regulations on how to transport these types of specimens. These are Infectious Substances category A specimens, which are very dangerous infectious material. We use appropriate, internationally-approved packages (Category A triple packaging with all its international requirements) to transport these specimens (Category A infectious substances with UN number 2814, meaning that they can infect both animals and humans) to laboratories that have the capacity to perform the required tests.
Now, how are these samples carried? I ask from a biosecurity perspective.
JBN: To protect the population, all specimens are accompanied by laboratory personnel. Official transportation is provided to ensure security.
A lab person that handles the specimen, and there is a driver to transport. But when the specimen is appropriately packaged, it should not be dangerous, and anyone can potentially handle the package without risk.
I have two more questions. One relates to infection control measures and the other to decontamination. What infection controls measures are put in place to ensure patient-patient infection does not occur, especially when you have virus-positive and “quarantined” patients in the same area?
JBN: The health workers to be trained on how to protect themselves, the environments, their patients and their families and relatives. Unfortunately healthcare workers are on the front lines of the disease and at risk of contamination. They have to be sure to follow the infection prevention and control rules by correctly wearing their personal protective equipment when examining or carrying for patients. They have to wash their hands, their boots, and everything, to ensure they are not contaminating the other wards.
Do you use some kind of cleaning solution?
JBN: Yes, that’s what we have; it’s very effective. The good news is that since the Ebola outbreak has been declared, we’ve had very few health care workers become newly infected. But, [prior to the official declaration of the Ebola outbreak], this outbreak was a disaster for health care workers. 26 were infected, 15 of whom passed away. This was the first time Guinea faced such a bad outbreak. And maybe it was different because healthcare workers did not know how to protect themselves, and they thought the disease was something like cholera, like meningitis. But this was something else. It was a highly dangerous, class 4 pathogen. It took a long time to make [healthcare workers] understand that the whole time they are taking care of the patient, they need to protect themselves—wear gloves, a mask, and even eye protection.
So had the healthcare workers just not received the right training, or were they new?
JBN: First of all, when the outbreak started, many did not know about [Ebola]. They thought it was like any other disease, like malaria. Some patients arrived at the hospital, bleeding (bleeding from eyes, ears, and nose is a late symptom of Ebola), and some of these patients were mistakenly operated on, which was a huge problem in terms of contamination of healthcare workers. But fortunately, now, things have dramatically changed. We no longer have as many healthcare workers that are getting infected, and that is thanks to information and training.
Do you know about how many have been infected?
JBN: Recent figures say that over 300 people [as of 10 June] have been infected since the start of the outbreak, and the mortality rate is about 70%. [As of mid-August 2014, over 2000 Ebola cases had been reported].
Is this mortality rate unusually high?
JBN: Not really. This mortality rate is expected for Ebola, especially as this is the Zaire Ebola virus strain, which has a very high mortality rate.
For more information about WHO-AFRO response efforts in the Ebola outbreak, please visit:
click here.
Please note: Outbreak numbers change quickly and the numbers cited in this interview may not reflect current estimates
- Quick link: ASLM Ebola Resource Centre
- To learn more about joining the African Public Health Laboratories Network (APHLN) Listserv, please click here for more information.
Dr. Paula Fernandes is the founder and president of Global Scientific Solutions for Health (GSSHealth). She is a medical laboratory scientist with more than 20 years in biomedical science, infectious disease research and international public health.